by Zowe Smith Published May 27, 2023
Part 1: The Before Times
IT WASN’T EASY TO REPORT JAB INJURIES IN THE ‘BEFORE TIMES’

It was rare for a vaccine injury to happen during my career as a medical coder but there were codes available should one occur. T36-T50 codes were on the books for poisonings and adverse effects of all kinds of drugs, including vaccines. T88.xxxx series is for reporting complications following vaccines. Instructions are very clear about side effects of any kind, even if it is considered normal, they should be reported. Rash and soreness at the injection site would be reported as a complication despite media screaming at us all day long that rashes and soreness is totally normal. Media also denies that vaccines can cause seizures and joint problems, yet there are codes for reporting “post immunization encephalitis” G04.02 and “post immunization arthropathy” M02.2. If these “side effects” don’t happen, then why do we have codes for them? CDC published 4 severity categories for vaccine adverse events and they provide a link to the VAERS website for reporting them.
Mysteriously, there is no mention of the ICD-10 coding system that the CDC and the WHO mandates healthcare systems to use. As a medical coder, I never received any training on reporting to VAERS. I never even heard of it until Covid-19. We were extensively trained on disease and drug safety reporting to CDC.
What would it take for someone to be labeled as a vaccine injury in the before times? Your provider would first need to recognize the condition they are seeing is related to a vaccine. Which is extremely problematic for a variety of reasons. Physicians are taught that vaccines are the best invention since oxygen. Coverage of possible reactions, side effects, adverse events and even death are completely omitted from their education. Leaving your medical ‘expert’ with a gaping blind spot when it comes to identifying vaccine reactions of any kind. How can your doctor know what symptoms could manifest after vaccination if they never even read the package insert? It’s the document intended to tell your doctor what to look for and what to do should you have a reaction. Pharmacists are the designated experts other physicians turn to when they need information on drugs. Turns out not even your pharmacist is able to advise providers on possible adverse effects. They don’t receive training on it either. We certainly didn’t receive training as medical coders or auditors.

When a patient walks in with a rash, for example, doctors are likely to suspect allergic reaction first. They look for environmental, chemical or food sources. Things like peanuts, detergents, and bug bites. Often, there is no identifiable allergen. I’ve seen it 1000 times. Patient walks in with rash and gets diagnosed with an unknown allergen. If physicians cared to look in their medical record, they would have found recent vaccinations in an awful lot of cases of young children with unidentifiable rashes. Patients get prescribed epipens, antihistamines, steroids, and antibiotics to treat their symptoms. Perhaps the most important medical advice is completely absent. Avoiding re-exposure to the allergen. By not identifying a vaccine as an allergen, it sets patients up for even more severe reactions next time.
In the rare moment when a physician does suspect a vaccine could be causing a bad reaction, there is a very strong tendency to deny it. Notes would reflect doctors documenting Gillian barre, which their patient suffered just days after receiving a vaccination, was “not due to the vaccine”. Gillian barre just “spontaneously” developed as an auto-immune version of the disease. Same situation with bells palsy. Debate ensues online if bells palsy is an autoimmune condition or vaccine injury.
One can begin to understand the incredible odds against reporting vaccine injuries long before Covid. The physician has to recognize it and write it down first. Adverse events were often mistaken as allergies or other diseases. When adverse events were identified, codes for reporting which vaccine was to blame were vague. Yet there was a framework available. Serum vaccines, viral vaccines, or bacterial vaccines. There are even codes for adverse reactions to immunoglobulin injections, pertussis and smallpox vaccines specifically. Researchers, Medicare, CDC and WHO pull medical records using these codes to monitor safety of all of them.
Part 2: Emergency Use Everything
UNSCHEDULED CODING UPDATES FOR EMERGENCY USE
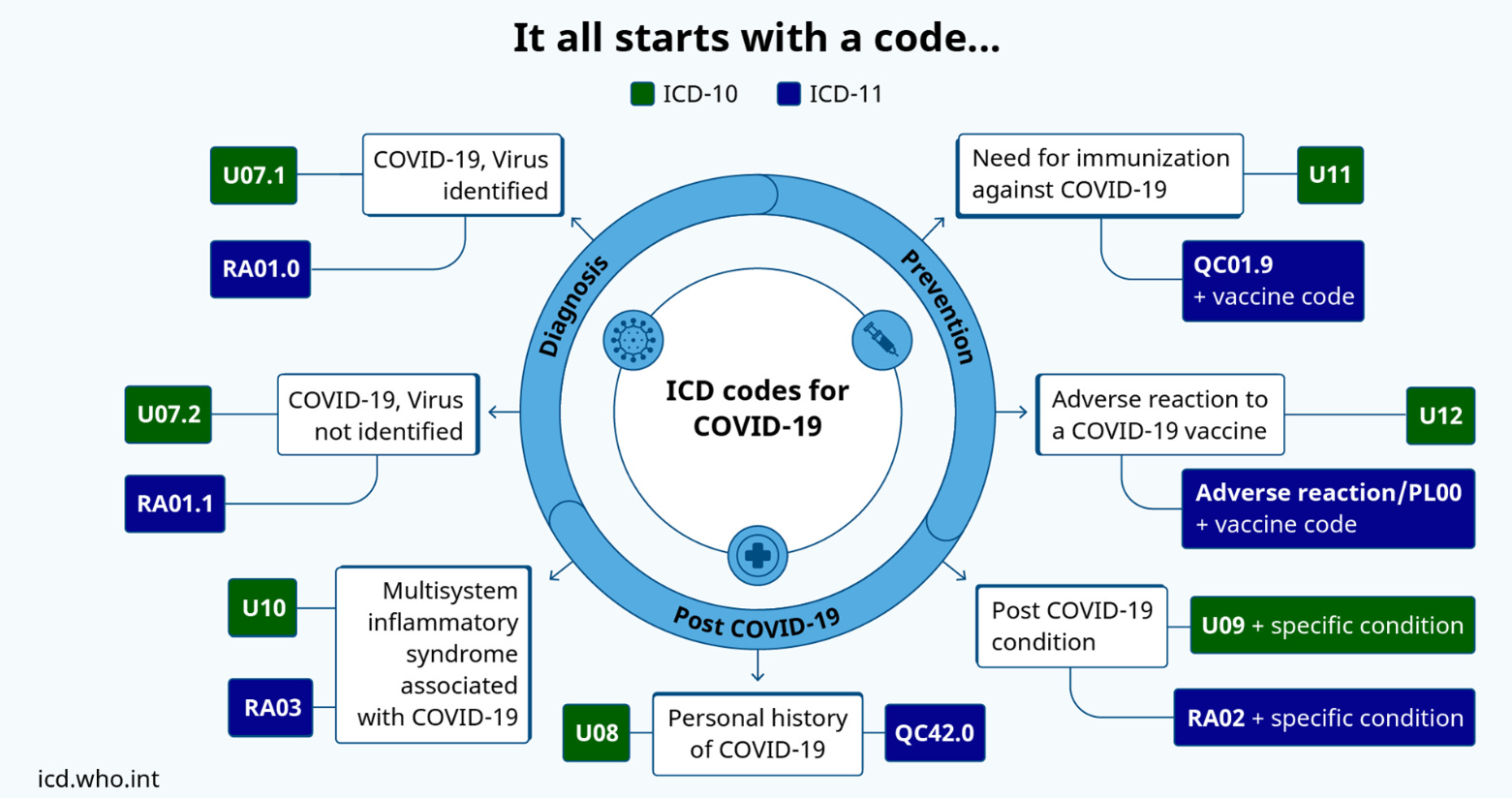
April 20th 2020 was the unprecedented day of an unscheduled coding update. The release of “the one code to rule them all” U07.1 Covid-19. It was for the sole purpose of introducing codes for tracking and reporting Covid cases using the ICD-10 coding system. The system that has been used internationally for tracking and reporting all diseases and causes of death for well over 50 years. With the update came an exception to viral infection reporting. After April 20th 2020, all a physician had to do was document they thought a patient had Covid-19 and that was clinically sufficient! No PCR test required, just the physicians medical opinion in written format, placed in the medical record. Suspiciously, the only other diseases to have this exception (section 2, H) were viruses Dr Fauci at the NIH had been involved in studying, HIV and Zika. Audit risk is extremely high when reporting a disease without clinical evidence to back it up, so these exceptions were almost never invoked. Instead, PCR tests were used to provide clinical evidence of infection.
The exception allowed, for the first time, a virus identifier code to be sequenced first. Coders were questioning this new coding advice because it was backwards. Virus identifier codes had no monetary value associated with them, and instructions said they could not be reported as a primary diagnosis. The primary diagnosis is the one insurance pays on. The first diagnosis is the main data point used for statistical reporting inside and outside the cult also. Before this update, a viral pneumonia case would be coded as pneumonia. A virus that causes a rash would be coded as a rash. Now all of these cases were to be labeled Covid-19 cases which would qualify for Covid bonus payments.
Not only was the new code U07.1 oddly supposed to be sequenced first but it wasn’t in Chapter 1: Certain Infectious and Parasitic Diseases (A00-B99). U07.1 Covid-19 wasn’t an A or B code as all other viral and bacterial identifiers are. There was room in the infectious disease chapter for code expansion, so it wasn’t as if they lacked room in the correct chapter. So why did they categorize Covid-19 as a U-code? Only someone who understands medical coding could even dream up such a question.
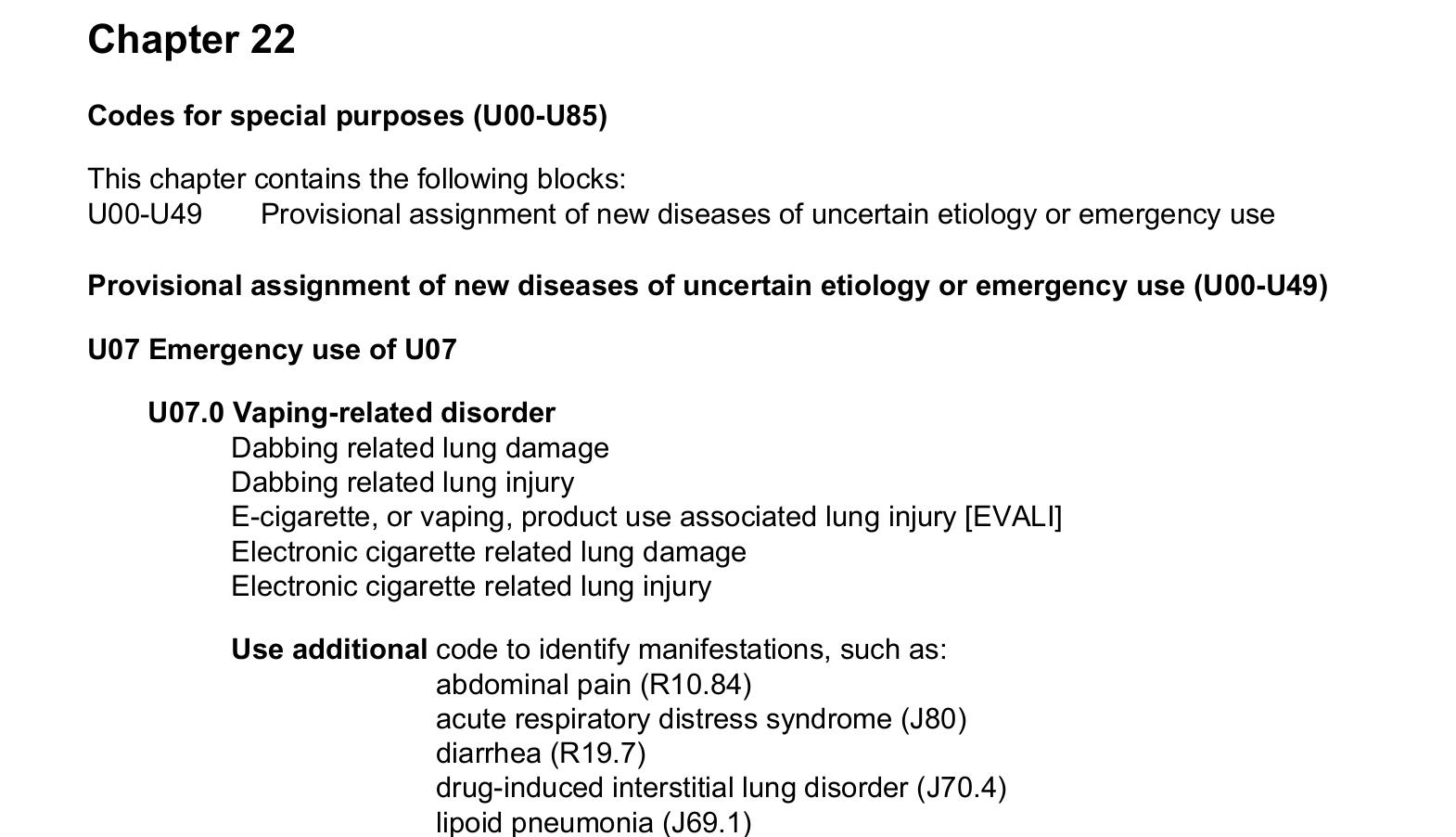
The answer is emergency use! The code U07.1 for Covid-19 is in the Chapter 22 (pg 101) Codes for special purposes and emergency use (U00-U85). In this chapter we find codes for EVALI, a vaping related lung disorder, Covid-19 and their term for long haul Covid-19.
THE AGE OF MEDICAL SURVEILLANCE

For the duration of 2020 media relentlessly repeated their mantra that a safe and effective vaccine was going to get us out of the pandemic. After nearly a year of anticipation of what operation warp speed would bring, the waiting was over. On December 6th 2020, the hospital I worked for began administering Covid-19 vaccinations via drive-through. If there were to be any new codes relating to Covid-19, this would be the time to release them. During research and development would have been the time to create them. Operation warp speed began approximately March 2020. Experimental Covid injections had been in development and trials for almost a year by the time experimental injections started going into arms. January 2021, just a few weeks later, was the next scheduled coding update. The alphabet agencies that created and maintain the ICD coding system had proven their ability to release new codes almost immediately. With a year of advanced notice, surely they would create all the necessary codes for reporting poisonings and adverse effects in the next scheduled update. It would even be close to on-schedule if they did.

Pharmacovigilince programs had been established for all vaccine trial participants and civilians alike. For up to the next three years. Vigilance programs were run by vaccine manufacturers using data collected from medical records. Tasked with finding safety signals in the data. The need for tracking experimental vaccine uptake was abundantly clear. How would we know we’ve reached herd immunity if we couldn’t calculate the percentage of vaccinated people? Contact tracing was well underway and a Covid-19 registry was in the works. Signs all around pointed to an overwhelming effort to track and record every potential data point around Covid-19 and ensure all that data gets sent to the feds. A precedent had already been set indicating if WHO thought a code was needed, they would create one.
Part 3: Lying With Statistics
THIS IS HOW THEY ARE LYING WITH STATISTICS AND HIDING GENOCIDE
Two years into the PLANdemic, there were countless cases of vaccine harm. Despite the most intense censorship I have ever seen, people began to talk about it. More importantly the barriers that I detailed earlier, preventing physicians from recognizing vaccine reactions, started to come down. Mind you not without breaking past incredible pressure. Physicians like Dr Zelenko, Dr Peter McCullugh, Dr Ryan Cole, Dr Paul Thomas were publicly smeared and/or lost their license for refusing Covid-19 protocols and reporting harm from vaccines.
As I noticed right from the start, the harm from Covid-19 vaccines was proving to be worse than all of the other vaccines before them combined. It was becoming so obvious it was hard to ignore. VAERS is the reporting system managed by the CDC for vaccine injury reporting. A system that is said to capture only 1% of actual vaccine injuries. OpenVAERS was created by the people in 2020 to reflect a more accurate number. As of May 12th 2023, 2.4 million Americans have reported injuries to OpenVAERS. 1.5 million of those were Covid-19 experimental injections. That is about half the vaccine deaths in America of all time due to Covid-19 vaccines. More recent studies are reporting even higher numbers using a combination of data sets from CDC, VAERS, HHS, Census, WHO’s Vigibase and publicly reported data sets around the world. They figure as many as 36 million global deaths from Covid-19 vaccines!
What data are researchers pulling to get these numbers? What evidence were injured bringing with them to the National Vaccine Injury Compensation Program? ICD codes derived from medical records and the records themselves. ICD codes (full version 2.1.2) that get reported more consistently than voluntary programs, like WHO’s Medisafe app. ICD codes typically get reported within a week of discharge. Obviously the well established ICD system would be more expedient and reliable than VAERS, Vigibase, or even Open VAERS. The problem was there was no way to report vaccine injuries specifically due to Covid-19 vaccines. Instead vaccine injuries were reported as symptoms or the disease injured patients presented with.
The coding world is one of specificity. When researchers pull ICD codes to monitor safety signals, the more specific the code, the easier it is to find relevant data. There is a popular opinion among coders. Nonspecific codes that lead to useless information are junk codes. Coders were at the mercy of applying junk codes for Covid-19 vaccine injuries. If they were able to report them as vaccine injuries at all. Why was there a code for Z20.828 Contact and exposure to Covid-19, Z86.16 (pg32) history of Covid-19, all the different brands of Covid-19 vaccines, other drugs used to treat it, even codes to track the unvaccinated (Z28.310) but still no code for vaccine injury reporting?!
WHO quietly released THE code “U12.9 Covid-19 vaccines causing adverse effects in therapeutic use, unspecified” in January 2021. Shockingly, the fine print advises not to use the code for international comparison. To certify a Covid vaccine death WHO physicians should not be provided a copy of the coding guidelines. Those guidelines would clearly walk physicians down a decision tree instructing them to report even the slightest vaccine effect as an injury. Instead WHO thinks it’s somehow more objective if physicians tasked with certifying deaths should be prevented from having all the information. Buried even deeper in the WHO’s update 3 & 4, they explain how the code U12.9 cannot be used because medical coding software has not been updated to include it! Something that could be easily remedied in the same way they did it in April 2020. April Fool’s day.
To claim they don’t have the ability to update software when we do it everyday could be translated as saying they just don’t want to. It’s passive aggressive speech meaning they don’t want anyone to know there is a way to report vaccine harm and if anyone figures out there is, they need to be in control of how it is used. Because that data would be a huge smoking gun pointing at them and they can’t have that.
Further, reviewing American and Canadian coding advice, coders have asked about coding adverse reactions to vaccines and their advisors do not point to using U12.9. It’s as if they don’t know the code exists. How could this be? It came to me when I recalled a coding consultants advice, Dr Z. He frequently said errata did not get published in official code books or in coding software. WHO’s update 3 & 4 has been largely unpublished. It was not publicized by any party in the cult. Similar to errata from AMA, coders had to know updates could be posted there and to check periodically. That is why U12.9 adverse effects of Covid-19 vaccines is not being reported.
In order to discover this key code existed, a freedom of information request had to be sent to the Office of National Statistics (ONS) in the UK. Not any of the traditional coding advisory boards or healthcare officials. The statistical office. They explain deaths are tallied by death certificates using WHO criteria. A follow up request was sent almost a year later asking to quantify and break down the deaths. Office of National Statistics, UK declined to provide any data citing section 22A and explaining their intent to publish their analysis in the future. The FDA in the US was a little more bold in asking for 75 years to analyze their vaccine injury data when pressured under their own FOIA request.
This is how they are lying with statistics and hiding genocide via vaccines from you on purpose. If you are good with excel, you can locate their monthly mortality report. It shows a breakdown of code U12.9 Covid-19 vaccine causing adverse effects was only assigned 18 times in 3 years!!! Adverse event reporting for vaccine injuries is buried under 3 layers of barriers and entirely at the discretion of the WHO. Imagine how much higher the number 36 million would be with every single medical encounter honestly and transparently being reported? We might not ever know. The WHO and their partners in crime saw to that.

Thank you for reading and supporting my work!
You were meant to be free,
-Zowe