Supporting a parallel economy, this is how we change the world
What makes it a Freedom Market, and why was this the perfect setting for the first book sale of The Covid Code My Life in the Thrill Kill Medical Cult? Glad you asked…
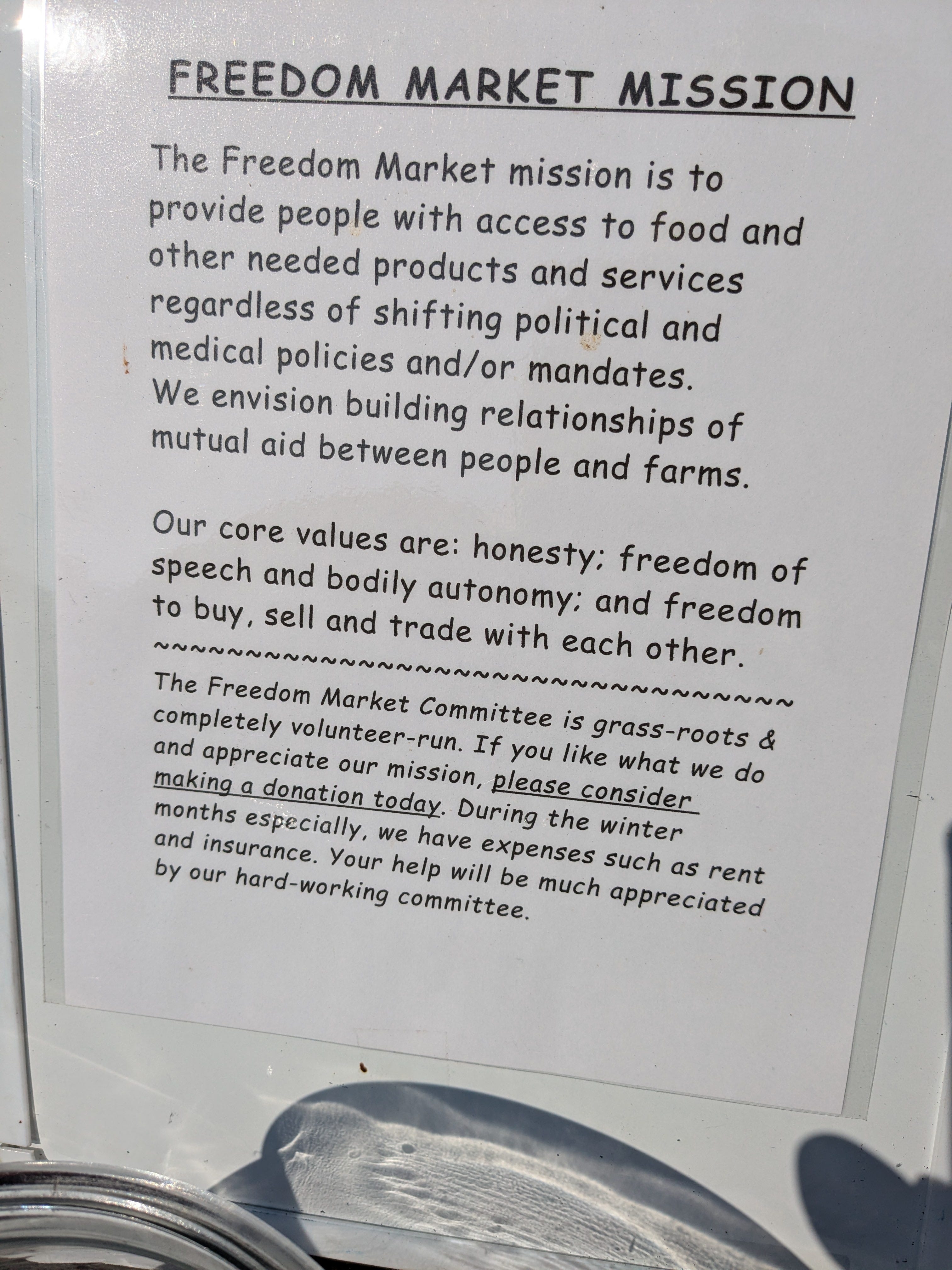
This market stands out because of its unique mission. First and foremost, since it was founded during the height of Covid hysteria, it shouldn’t surprise you that being able to attend mask and vaccine free is a core value. As are respecting bodily autonomy and freedom of speech. One woman who organizes the market explains, “We are free from the new world order”. If you aren’t familiar with that term, you have some catching up to do. Simply put, at this market, nobody has to ask for permission to sell from the state. Nobody has to pay for licenses, permits, or inspections. There are no regulations to dictate what products are safe to consume. Regulations that would normally prevent selling veggies to a neighbor, raw dairy consumption, unpasteurized apple cider, and meat that has been home-grown and processed. Vendors are also free to accept alternative currencies like silver and gold, free from tax and tracing. Don’t let the lack of regulations fool you; each vendor is a craftsman in their own right. Held accountable by high levels of integrity and a sense of duty to provide a useful service to the market community.
The freedom market might be the only one where you will regularly find other people as passionate about exposing the ongoing mass genocide, as myself. It continues to amaze me how people in the freedom and truth communities miraculously find each other. Giant bumper stickers like this one that reads “Covid-19 hospital protocol kills” might earn you serious harassment in the wrong crowd, but they quickly bring together the awakened ones. In these days of psychological warfare and intense gaslighting, it’s always nice to know you aren’t alone in recognizing that the media is the virus.
Can you imagine someone walking up to the genocide syringe mobile and asking to get the jab? True story: it happened. The person asked if the driver was handing out jabs that day because she still had room on her vax card for more. The driver of the genocide syringe mobile was speechless. It is tragic how these vaccines are murdering innocent people, but at some point you have to wonder about the blind order followers. In lemming society, those individuals would be the first to jump off the cliff.
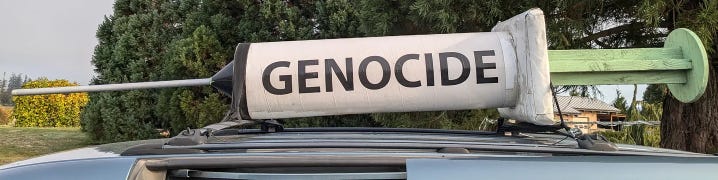
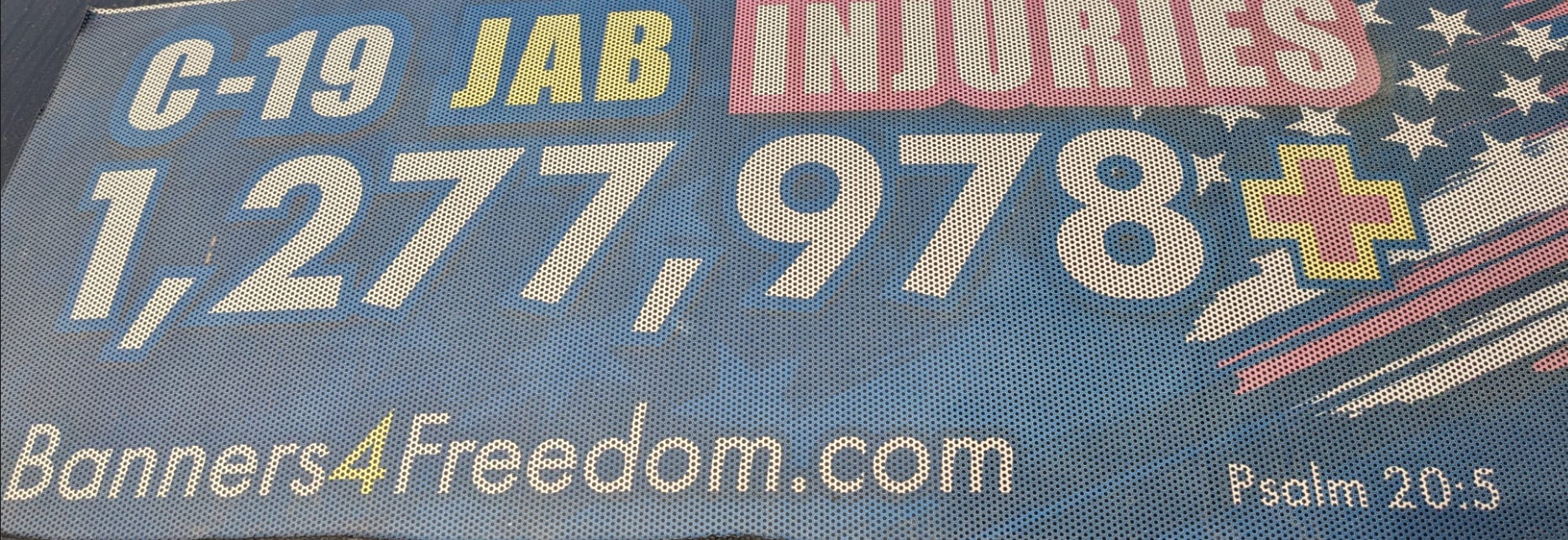
The vaccine injury tally continues to grow, as does the number of banners available. Check them out here and start educating your community about the invisible genocide and other censored topics at banners4freedom.com. Be like the legendary woman who drives the genocide syringe mobile!
It’s no secret that I have been called toward farming since leaving what I now refer to as the medical cult. Being born and raised as a city girl and growing up as a genuine tree hugger would suggest it is an unusual move. Environmentalists and conservationists tend to look down upon farming as a source of pollution. Farming has been vilified because of the heavy use of industrialized practices. If Covid taught us anything, it is that the chosen narrative is never what it seems. Farming is no different.
On my path to heal myself, after I had exhausted what western medicine had to offer (you can read about it in chapter 5 of The Covid Code), I turned to organic, unprocessed food. Only to find out grocery stores don’t sell that. They buy in bulk from farmers in faraway lands and use deceptive labeling to convince you to pay extra for ‘farm fresh organic foods’ that are tainted or poisoned in various forms. The best way to know what is in your food is to grow it yourself; the next best thing is to buy it directly from the farmer. When I began asking farmers about their growing practices, I learned they were just as concerned about the health of the environment as I was. Better still, there are farming practices that do not require fertilizers or pesticides. These alternative practices build up soil health and produce more nutrient-rich food.
When you consider that my family line was all farmers until two generations ago, the transition back to the land begins to make sense. There is just one problem: the mass genocide by hospital protocol and vaccine injury needed to be exposed. Getting back to the land had to take a back seat until my mission was complete.
Thanks for reading My Life In The Thrill Kill Medical Cult! This post is public so feel free to share it.

After two long years of writing, The Covid Code is published and ready for sale. That may seem like a short period of time to some authors, but the rush to get the messages in this book out to the public cannot be understated. The healthcare workers who remain in the system are the ones who will follow protocols without question. If hospitals became kill centers during the scamdemic of 2020, the groundwork is laid for a much worse story to play out if there is ever a rerun. This book may contain keys that will help people fight back if that ever happens, or possibly even prevent something like Covid from ever happening again. It may help people who have lost loved ones understand the sinister motivations behind their murders. Most of all, it will instill doubt in the healthcare system as a whole. The medical cult has worked for decades to prevent anything from making the public doubt or distrust the modern healthcare system. It just so happens to be my mission to affirm that distrust. What better place to start than with a group of health-conscious people?

Wonders of alternatives to modern healthcare abound. There are herbal teas, tinctures, and salves in every color and variety. Natural and ancient food remedies are also for sale. There are over 74,000 ICD-10 diagnosis codes in the international classification of diseases that the WHO manages. Remedies from nature are just as diverse. Everyone’s biochemistry is unique, and so are the options one can use to manage them.



The freedom market has been running for four years strong. It hasn’t been easy. Community leaders and organizers always need help finding suitable market locations. As a grassroot, volunteer run market, donations are always needed to assist with overhead costs. Where there is a will, there is a way. This group of dedicated people wants to create a better future for themselves and for their children. They understand it takes small strides like this to get there. Forming a network of people who can provide the supplies you will need for survival if all other options get cut off is great. Worth its weight in gold is knowing that the community will be there to help you if disaster strikes. Wouldn’t it be wonderful if you knew your neighbor would help if your house burned down? Or if you needed a hand with a barn build or help to bring in a harvest? Wouldn’t it be great if you had that kind of sovereignty and confidence? The freedom market is trying to model that future for us all. This is how we change the world.
Anyone can organize one of these markets. Every town needs one to call their own. If there is one near you, go and support your neighbors and local farmers. Get to know them. If there isn’t one in your town going already, that is your cue to start one. Talk to your neighbors and see if there is any interest. Schedule a gathering to talk about it at a local establishment. You might be surprised at how many other people want to do the same thing, but they just don’t know how to get started.
Memory Lane: The First Market
The journey I took to write The Covid Code was far from traditional. Perhaps that will be the topic of a future article. When Covid vaccine mandates threatened to remove my primary and backup careers, I had to make some major life changes fast. On the VAXXED bus, I mentioned that I haven’t worked in three years. That means that I haven’t been able to earn an income since April 2021. It is not for lack of trying! There have been various farm jobs that all fell through quickly. Countless applications have been submitted only to find that I am overqualified or underqualified. At one point, I opened a paleo bakery called Rebel Grey, and I held a booth at the very first Freedom Market to promote it. Killer baking skills aside, the market demand was not there for the products I was selling. Barriers to entry were too high in the remote area where I found myself living at the time. The decision was made to close the bakery and focus on writing.

If you are interested, here is a short video from the very first freedom market, where I sold baked goods instead of books. Watch the video

Stretching after a long day of meeting new friends and spreading the truth. Until we meet again.

T SHIRT SHOP (All designs now available in black except hoodies)
You were meant to be free!
-Zowe Smith