Part 1: From Contact Tracing to Gene bank AI “Ecosystem”
Medical Surveillance
Part 1: From Contact Tracing to Gene bank AI “Ecosystem”
JUN 13, 2024

Unedited Version
Originally Posted on The Last American Vagabond Substack on May 31, 2024
For more info and news go to The Last American Vagabond website
**AUDIO RECORDING ONLY AVAILABLE AT zowe.substack.com**
BIG TECH BROUGHT IN FOR CONTACT TRACING
You may recall, early in the scamdemic, all the rage was about contact tracing. Public health officials advised Covid-19 could be spread by people who didn’t have symptoms for up to 14 days. Anyone who had been within six feet could be contaminated and unaware. Hospitals began questioning patients about their contacts. For the first time, personal information and that of their contacts, with was recorded.
This was not normal practice for other infectious diseases. It was normal to ask patients who had HIV about their partners. To my knowledge, it was up to the individual to tell those partners. Their contacts personal information did not become part of the record. The HIV patient’s data would then be de-identified and sent to a CDC database for disease surveillance purposes.
Social workers were brought in to help collect data for Covid-19 contact tracing. It was a tedious task that would not be sustainable without digital assistance. As early as April 2020, contact tracing had been outsourced to big tech. Smartphone apps for contact tracing were stealthily released through a regular update. Apple and Google claimed it was strictly an opt-in program. Anyone who updated their phone was passively being tracked via Bluetooth. The only difference was that people who chose to participate got notifications when they were within six feet of a Covid-19 case.

BURNING THE FIREWALLS TO VIOLATE YOUR PRIVACY
Collecting the medical record data was sure to go through the American Hospital Information Management Association (AHIMA). They are responsible for licensing medical coders and other health information professionals. It is the responsibility of AHIMA to manage contact tracing data submissions. It also falls on AHIMA to regulate Covid-19 data submissions to the CDC.
In their journal, I learned a disease registry for Covid-19 was being created through a partnership between labcorps and CIOX. Labcorps was one of the first public labs to roll out Covid-19 PCR testing. It was a perfect match, with Lapcorps providing access to test results combined with COIX’s data integration software.
A Covid-19 coalition was formed with the stated purpose of sharing and leveraging real-time data. When I put together the members of the Covid-19 registry and the coalition, I began to see how alarmingly public our private medical data has become. Some members of the coalition overlapped those of the registry; Amazon, google, and Microsoft. Some members like Palantir, MITRE and In-Q-Tel clearly represented the interests of government intelligence agencies.
When I became aware of this in early 2020, I was not the only one concerned with the massive amount of data being collected on people without their knowledge. Some parts of HIPAA, the law that is supposed to protect patient privacy, were waived to permit information sharing. More concerning still, this information appeared to be shared with big tech and government intelligence agencies. Instead of calming my fears about private medical data being shared, AHIMA was adding fuel to the fire.
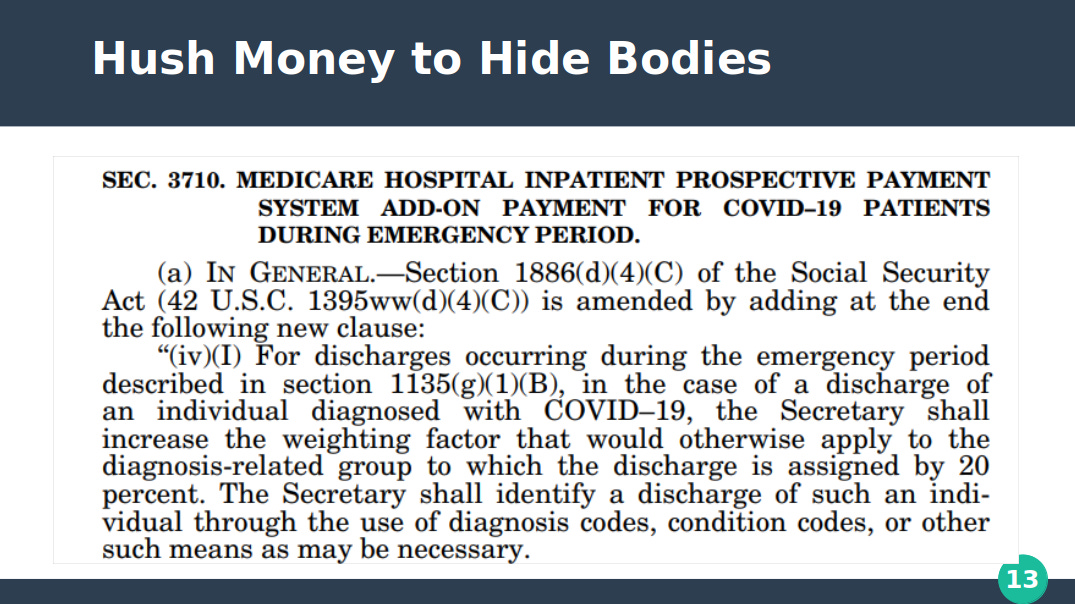
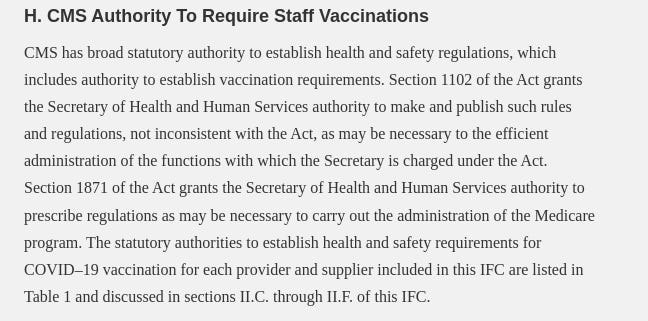
I was unaware there was a program that required hospitals to send patient data to HHS at scheduled intervals. It was part of the HHS protect system. That kind of data transmission was above my pay grade. I was occasionally clued in if the transmission failed. I would overhear grumblings about how the hospital wouldn’t get paid if tech support was unable to fix it in time. I didn’t understand Medicare could reduce payments if hospitals failed to send the required information. The HHS protect system replaced The National Health Safety Network. It is the program Medicare exploits to tie funding to healthcare staff vaccination compliance.

AI IN ELECTRONIC MEDICAL RECORD SOFTWARE
It was shocking, to learn the 3M program I used as a medical coder, had AI built in. How did I not know this? The program had a feature called computer assisted coding. It used natural language processing to analyze records and predict ICD-10 codes. My job as a 3M trainer was to teach coders how to correct the auto-predicted codes. The more coders fixed errors, the machine learning feature would improve code predictions. The big wigs told coders the program was a tool to improve efficiency. In fact, it has been slowly taking over coding jobs as its usefulness improves.
The other program that dominates the electronic health record market in the United States is EPIC. Many hospitals use this program as their core electronic health record system. I learned during the scamdemic that EPIC has multiple AI features built-in as well.
The latest development in healthcare data integration is adding an AI listening feature to generate notes. 3M partnered with Amazon, a member of the Covid-19 information sharing coalition, on the project. The AI listening feature will be integrated directly into 3M. The program will listen to the whole conversation, and doctors will only have to approve the AI-generated note. This is a step ahead of EPICs dictation software, which operates a lot like talk to text on a smartphone. Physicians can also draft templates in EPIC and edit the variables. Either way, the downside is the doctor has to devote additional time generating the notes. EPIC is getting on board to solve this by integrating AI listening features into its software as well. The privacy concern with that is every computer in the hospital is always listening. This effectively kills any facade of privacy in healthcare.

PALANTIRS TENTACLES IN HEALTHCARE DATA
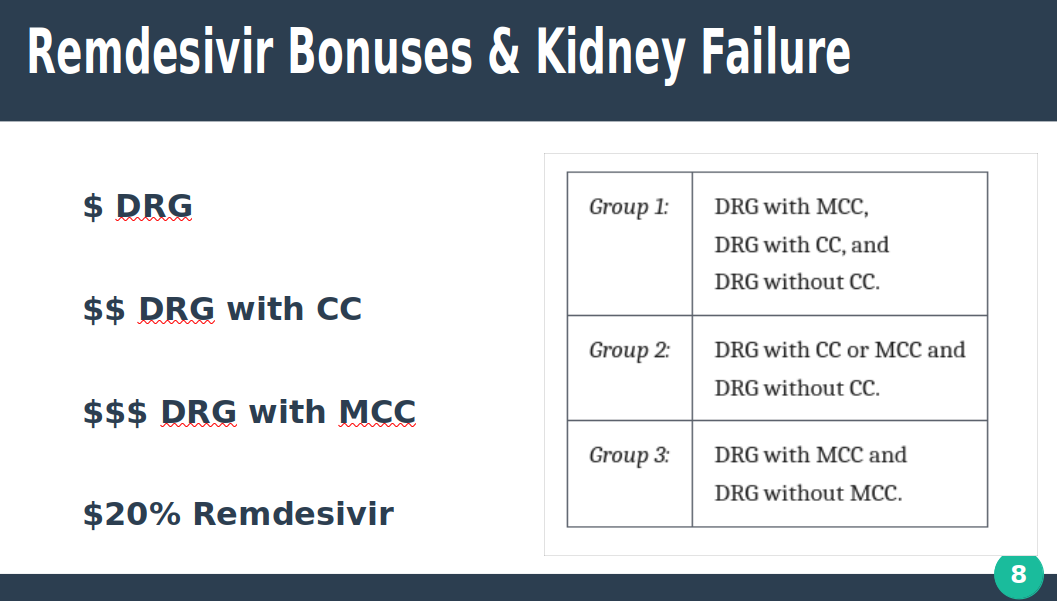
Palantir has a heavy hand in merging AI with electronic healthcare records or EHR programs. Palantir was contracted by the CDC to build a contact tracing app. For Operation Warp Speed, Palantir provided an artificial intelligence program called Tiberius. It was supposed to monitor the ICU bed capacity and ventilator availability. It layers 225 databases across the public and private sector and places them into one “ecosystem”. Tiberius can target ethnic groups based on risk behavior and location. It doesn’t just map data, it can predict behavior. Palantir was a member of the Covid-19 registry and information sharing coalition. Palantir also provided the AI platform used by HHS protect to distribute Remdesivir, the deadly drug that causes kidney failure. Not only that, Tiberius was also used to identify patients for vaccine clinical trials.
The CDC commissioned their contact tracing app with Palantir. It was later revealed contact tracing data was collected on Americans without their knowledge and used to give them an infection risk score. The CDC and Department of Homeland Security also purchased cell phone data to monitor lock down compliance, among other reasons.
Palantirs desire for data surveillance shouldn’t be a surprise, as the company was born from a failed CIA program called Total Information Awareness that was privatized. A look at Palantirs partnership with DARPA, In-Q-Tel, and the CIA confirms their roots in intelligence.
I found it disturbing that the other members of Palantir were software companies that developed the programs that were used in electronic record management and medical coding. They were EPIC, 3M, Optum, Allscripts, and McKesson. Every hospital system I worked for used at least one of those medical record systems. In order for these companies to work with Palantir, contracts are required that permit information sharing. An insider who formerly worked at the software development level at 3M, explains the information sharing that happens “is far more than you know”.
THE PUBLIC-PRIVATE PARTNERSHIP VIRUS
The Covid-19 registry has been disbanded since HHS declared the end of Covid on May 11, 2023. Since then, all the links and references I saved lead nowhere. Registry members were agencies like the National Cancer Institute, NIH, NIAID, National Academies of Science, and Research Alliance Group. Not surprisingly, the Covid-19 vaccine manufacturers were members. The tech companies building the infrastructure were Amazon, Palantir, Google Cloud Services, and Microsoft Azure. Government and intelligence agencies were also noted as members. Any mention of DARPA, the CIA, or the Chinese governments involvement, has vanished without a trace.
As often happens, the Covid-19 registry database was absorbed into a private company. CIOX was acquired by Datavant. The Covid-19 registry has been integrated in Datavants real-world data AI ecosystem. There are over 500 partners that continually feed data into the ecosystem which can be used by all partners. Private patient information is de-identified in the ecosystem. Government agencies are allowed to see individually identifiable data, however, because they are exempt from privacy laws.
Healthcare systems partnered with China for Covid-19 research purposes during the pandemic. This granted them access to American healthcare data. The most valuable data is our DNA. As Karen Kingston (and Derrick Broze) points out, the Chinese government acquired Americans DNA under the guise of Covid-19 PCR testing.
BGI is China’s leading genomic company. They have been busy building a gene bank for a very long time. It started out for the human genome project. Like Datavant, BGI partnered with American tech companies to build the gene bank. Their goal is to be able to identify how individuals respond to viruses and vaccines. During the pandemic, BGI sold American providers, like labcorps, Covid-19 PCR test kits. Perhaps that is why the CDC required labs performing Covid-19 PCR tests to send genomic sequences to them. Labs were further instructed to upload the genomic data to public gene banks GISAID and NCBI. This is how our genetic data has been collected and uploaded into a public gene bank without our knowledge and how that information is shared with China.
MEDICAL SURVEILLANCE GOES UNDER THE SKIN
During the pandemic, the CEO of the hospital I worked for announced that city wastewater treatment plants would be equipped with Covid-19 PCR testing technology. It was proudly proclaimed as a way to predict pandemic outbreaks and monitor Covid in real time. As author Whitney Webb puts it, “under the guise of fighting Covid-19 [the medical industrial complex] increasingly seeks to monitor what is going into, out of, and happening within our very bodies.”.
I had to agree, it seemed all the tracking and predictive AI programs were leading into dangerous medical pre-crime territory. Private medical data is being shared with international government and military agencies. DNA is being collected from the public to create a gene bank without their knowledge. The information is used by governments and intelligence agencies to predict behavior and target ethnic groups with countermeasures like Remdesivir and vaccines. What could go wrong?
In part two of “Medical Surveillance” we will take a look at how the same AI software was used to develop a vaccine passport system. You will also discover how vaccine status is being tracked via the ICD-10 codes. Stay tuned because where this all leads is more explosive than medical pre-crime.
Other places to find me:
How to support my work:

Z28.310 is the ICD-10 code for being UNVACCINATED!
“You were meant to be free!”
-Zowe